

Introduction
This survey was designed to evaluate the impact of pilots of “CME databases” that the Welsh Government have been running in one-third of Welsh local authority regions over the last year.
These database mechanisms involve sharing identifying data of children from NHS healthcare sources without knowledge or consent of children or parents, with councils.
The purpose of those databases was given as identification of children by the council so that they can consider whether they are home educated or missing education, although the Welsh government subsequently claimed that these database pilots and the associated mechanisms would not relate to or impact home educated children or young people. (More can be read on this here).
This pilot has not yet concluded. However, for reasons that they have not disclosed, the Welsh Government brought forward the publication of their commercially commissioned evaluation of these “CME database” pilots to coincide with the closing days of the present Senedd term.
We were aware that no home educators had been allowed to be involved in the evaluation of the impact of these pilots.
We were also aware of the highly questionable methodology, content and extrapolations of the evaluation of their EHE guidance that the Welsh Government had commissioned from the same commercial company, which was published only weeks before.
We therefore undertook this brief survey of lived experiences of those impacted by the methods used in these CME database pilots, including of related experiences of non-consensual datasharing. This ongoing study was conducted urgently because of concerns of uncertainty of why publication of that evaluation had been brought forwards within the closing days of the present Senedd term, including concerns of triggering of policy enactments without full evaluation of risks, impacts and consequences of these, without engagement with the community, with experts in ethics, or with clinicians and professional medical bodies.
Methodology
A survey including multiple choice questions and numerous opportunities for free text written responses was developed, to allow production of quantitative and qualitative data. The range of questions were drawn from a spectrum of suggestions and concerns expressed in a variety of home education groups. The survey used Google Forms and was circulated via a range of Welsh national and local home education groups.
Due to time limitations, with the publication of the Welsh government’s evaluation being brought forwards to days before the close of Senedd business, this is an initial release of results from the first 4 days of the survey, as of 25th March 2026.
Responses were fully anonymised, with no collection of email or IP addresses.
Demographics of Respondents.
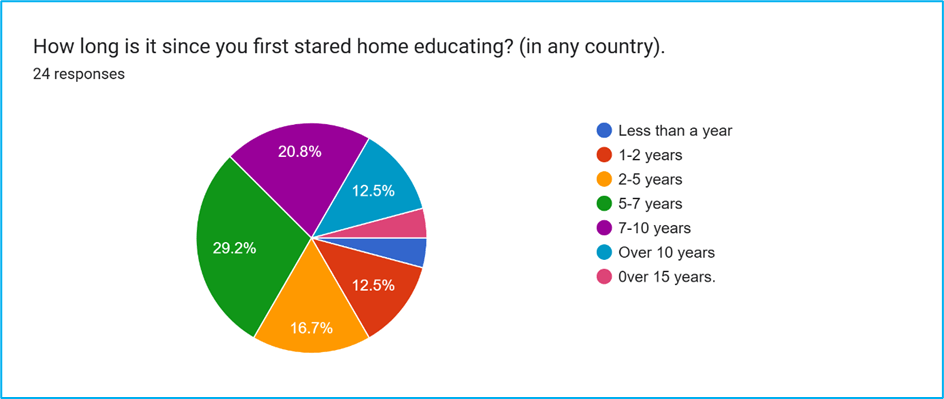
24 responses were obtained over a 4-day period. These were generally experienced home educators, with the duration of their home education experience demonstrated in Figure 1.
13 out of 24 respondents lived in areas where the council is participating in Welsh Government’s “CME database” pilots.
Results
Question 1: Results shown in Figure 2:
Nearly half of respondents did not know how the LA obtained their identifying data. Only 25% felt confident that they knew the source that had shared their identifying data.
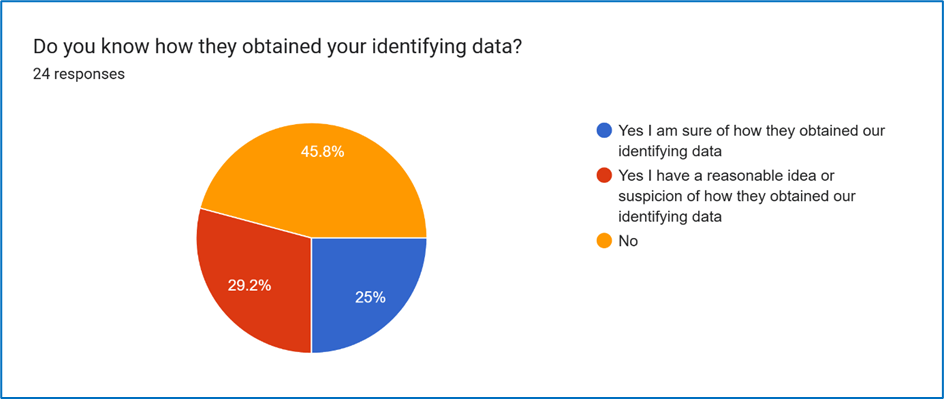
Figure 2.
Part of the difficulty of evaluating the impact of these database pilots is the lack of transparency by the council and lack information for families to know if they were identified as part of the pilot or by other means.
However, it is reasonable to believe that the key impacts of being identified because of data being shared from healthcare sources without consent are likely tb be very similar and equally relevant whether information was shared as part of this “pilot” or not.
Question 2:
Respondents were invited to comment further on their understanding and experience of the likely source of their data.
Concerningly, several respondents stated that they were cold-called by those claiming to be council staff but who did not know the children’s names.
This included respondents within pilot areas where it was considered likely that they had been identified by the CME database pilot mechanisms, including where only one sibling in the family had been identified by that mechanism. This mirrors the observations in the WG-commissioned evaluation of these pilots on the unreliability of source data used in such pilots.
It also demonstrates a significant safeguarding risk in terms of practice being established for it to be considered acceptable or normal to respond to strangers coldcalling and asking or “fishing” for information about children in this way
Some respondents, who lived in areas where the pilot schemes are running, were aware that they were identified because of this, although they were not necessarily told this by council staff.
For example they had to submit freedom of information requests to establish this, or they concluded that this appeared likely to be the source, having learnt about these pilot schemes from home education groups, having not received any information on these pilot schemes from their council or from the Welsh Government.
Two of these responses were from respondents in the same pilot scheme area but where the respondents felt it was clinicians who were responsible for the breach in confidentiality.
It’s a guess, but I had a hospital appt for myself, and my children came with me. The consultant was asking about why they’re not in school, and I explained they’re home educated. Never heard for LA until after that appointment, when the CME person randomly showed up at my door. They did know my children’s names, which wasn’t mentioned in my hospital appt, which is why I can’t feel 100% certain that that’s where it started. But it’s a bit of a coincidence.
They phoned my husband and the only number he has associated with our child is from a recent Dr’s appt he had taken her to where he gave his contact number. The rest of the contact numbers on any forms for our child are my number. (firstly it was the CME team, who then passed the info to the EHE team who then emailed).
Other responses indicating NHS sources for their data were from respondents who do not live in pilot areas:
Health visitor for younger sibling (not pilot area)
I don’t know for sure. But they door stopped us and asked about my youngest son (who has additional needs) but didn’t have any idea about my eldest (10). So I assume the prompt came from my youngest son’s medical interactions? (not a pilot scheme area).
Visited our GP when my son was unwell and she asked about school. We said he was home educated. The following week we received a letter from the school nurse saying we must ‘urgently’ contact them (this was even highlighted with a marker pen) to confirm what school my children attended. I asked advice from a (home educating) friend who works as a school nurse and she said that the service is optional so there shouldn’t be any need to contact them. A short time later we were contacted by the LA saying it had been brought to their attention that the children weren’t registered at a school.
Either from our health visitor/GP or from a local toddler group I attended with my now 4year old.
I had a phone call from ******* Hospital’s children’s department. They asked where he went to school. To clarify we’ve never (thankfully) had to visit the hospital/ children’s department.
We registered my youngest at the GP. I had left it until he needed to see the GP and already registered the rest of the family as he’s the only one who is still home-ed. The rest are now in college and university. Anyway, there was a question about which school he goes to which I thought irrelevant. I left it blank. A week later, I received a letter in the post from the health board stating that information was missing from his records. School he attends was highlighted in yellow. I once again ignored as it’s irrelevant. I was contacted via WhatsApp by the EHE department within weeks.
4 responses raised the possibility of non-NHS sources having shared their data without consent, for example a Steiner school, even though the child was not of compulsory school age, or social services following a malicious referral that was found to have no basis.
Several respondents indicated they had no idea how they were identified as home educators by councils, comments included that the LA would not tell them where they had sourced their data from.
Questions 3 and 4: impact on trust in councils and healthcare
The damage to trust in both council and healthcare staff by such datasharing was clearly evident, as demonstrated in Figures 3 and 4
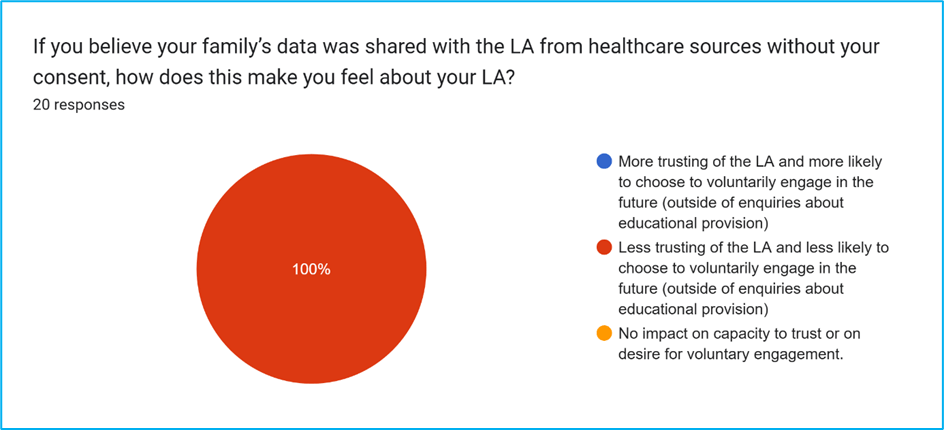
Figure 3: impact of non-consensual datasharing from healthcare sources with councils on capacity to trust councils.
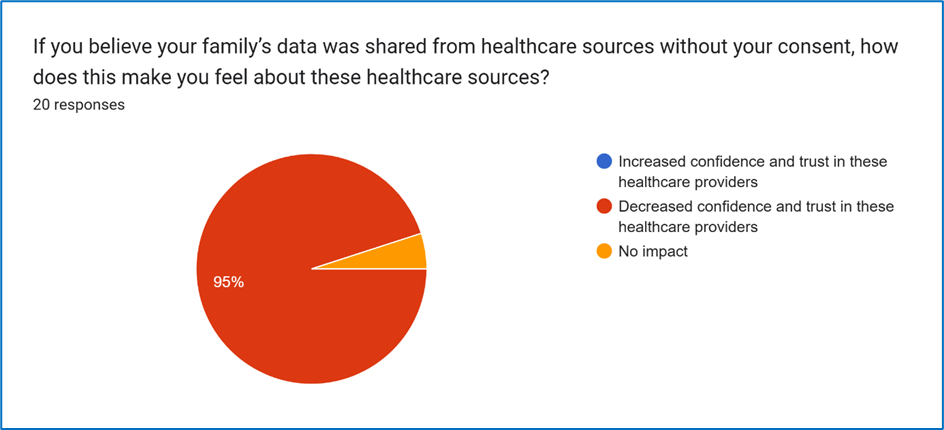
Figure 4: Impact of non-consensual datasharing from healthcare sources with councils on capacity to trust healthcare providers.
Question 5: impact of data being shared from healthcare
Respondents were asked:
If time permits, please explain your experience and feelings further in relation to your family’s data being share from healthcare sources with the LA.
The extensive responses can be most simply appreciated by consideration of phrases such as:
very upset
feel very judged
yet treated with suspicion as if it’s a police check
it feels very invasive and wrong
feel violated
all caught me off guard
didn’t know why they were phoning
definitely felt more wary
it would be a complete breach of trust
really saddened me
came from a time of scariness
that scary time was taken as an opportunity to report me really disappoints me, really makes me angry
I was, and still am, absolutely fuming
feel so, so angry about this
shared without consent
do not believe data should be shared without consent
Do not trust in competence of LA to safeguard confidential information – as evidenced by getting name wrong
No trust in official departments as result
They have also shared my email address amongst colleagues which also angers me
Requesting an annual report for her, as they had obtained her data from an unknown source…I reminded them she was three at the time
The doctor patient confidentiality should be sacrosanct unless there is genuine concern for the safety of the child
Home education is not a safeguarding issue
I will definitely be less inclined to engage with healthcare providers & the LA in future as a result
terrible idea to share healthcare data
It would reduce my trust in the healthcare sector as I wouldn’t feel confident in my data being protected and would be more reluctant to answer questions or divulge information during consultations.
Questions 6, 7 and 8: how council staff made initial contact:
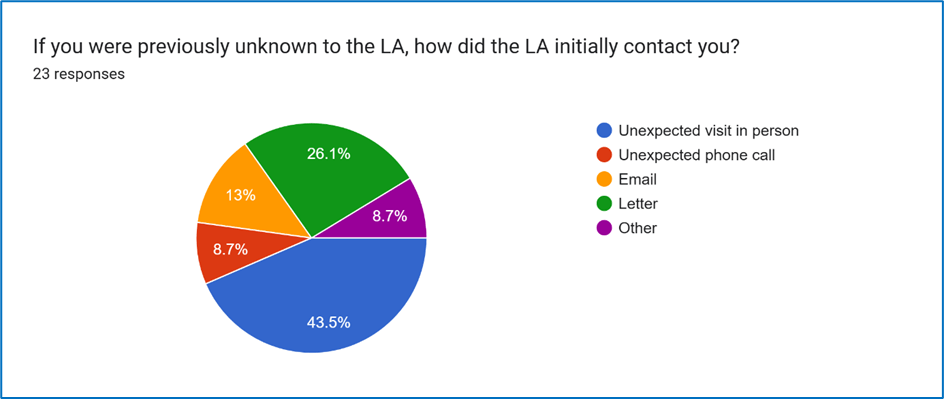
Question 6, Figure 5:
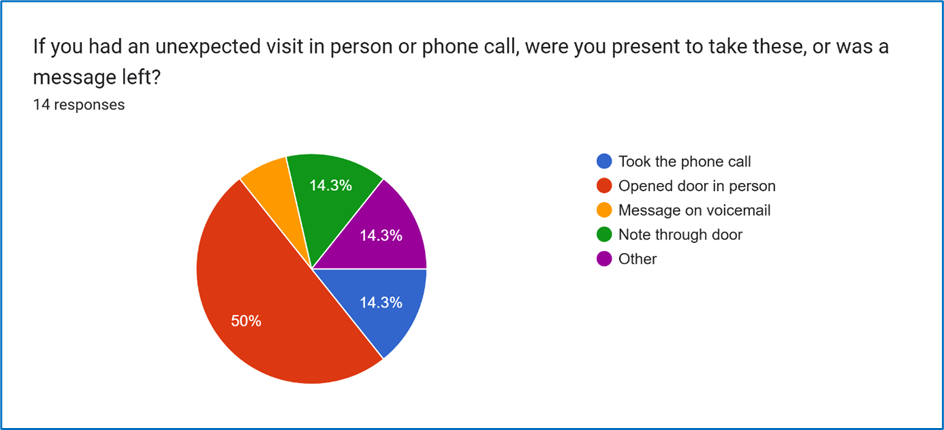
Question 7, Figure 6:
On over half of occasions, council staff chose initial modes of contact that would put families “on the spot”, rather than modes of contact such as email and letters that allowed time and opportunity to consider appropriate response.
Such unexpected modes of contact were received (by opening the door or taking the phone call) in 64.3% of cases.
It is noteworthy that all other cases, the council staff were equally able to make contact with the family. In person visits or unexpected cold-calling phone calls are demonstrated to not be necessary to establish contact with families.
Question 8: experiences and impact of initial unexpected contact, including the mode of contact chosen by the LA.
Responses included:
It made me anxious. I suffer with anxiety anyway just by someone knocking my door- this is due to an abusive ex turning up at my door unexpectedly a couple of times Also, due to how his family would make false reports to social services and the police, resulting in many welfare checks. So just a knock at the door makes me anxious. For it then to be someone in authority sent me into panic mode- due to the ex and his family and the things they did, I spent years being terrified my children would be taken from me. Every person who can impact my children’s life is seen by me as a potential risk to my family unit. They’re thriving in home ed and the thought of them having to go to school or having to keep proving to someone over and over, that I am meeting their needs is deeply unsettling.
An unannounced and unexpected doorstep visit followed by EHE bod showing up at our home for an appointment that we weren’t aware of, due to them sending emails to a miswritten email address. This has left our family anxious and concerned of ‘overstepping’ by the LA.
We felt anxious, like we were being identified/treated as if we were doing something wrong and now things were going to kick off some sort of official and invasive investigation.
Absolutely disgusting that they thought my child was missing in education
I felt like I was being hounded by them. Doorstepped twice in about 3 or 4 days
Was upset but it’s been fine (since)
It was shocking. I had no idea they would just show up at my door, asking ‘do XXX and XXX still live here?’ (like where else would they be?!) And actually without really doing a proper introduction first. To then say they’re from the children missing education team, and asking why my children are not in school. I explained home ed, and she just ok thanks, and left. No explanation. No letting me know what will come of it. Just…. Nothing. No warning ahead of time, and no letting me know what’s next.
Shocked and very stressful on us as parents.
My child is autistic & reacts strongly to any sense of their boundaries being breached, had they been aware of this visit, they would have been distressed by it & it would have decreased their sense of safety & control in their environment. I personally consider it incredibly rude to turn up to someone’s house unannounced in some kind of ‘gotcha’ moment as if they were somehow doing something criminal they needed to be caught out in. I am extremely unhappy that anyone with a lanyard could turn up unannounced demanding information on my child, it is damages trust & puts children at risk that this could set a precedent.
A letter would have been more professional. Luckily I missed the 1st call as was in work so was expecting it when they called again & was therefore able to explain I wanted everything in writing without feeling put on the spot which I would have done had I answered the 1st call
Unfortunately, the LA overstepped asking for information that they were not entitled to. This is why everything will remain in writing.
I was glad that they rang rather than doorstopping like they did to our friend in ****** , but I would have much preferred a letter of first contact.
This was disturbing and bordered on harassment of me and my family as the note was threatening
I was confused and annoyed at them having her data and also requesting information on her education before she’s even CSA. I felt like our privacy had been breached.
Pushy, unnecessary and invasive
We are a neurodivergent family. We don’t deal well with unexpected people contacting us. If they hadn’t written, I would probably have not picked up as I do not recognise the number. I prefer not to communicate by phone anyway.
My children were concerned they would just turn up on our doorstep (as they had done with friends). It made me feel very anxious and depressed. I think the letter was very unprofessional, it gave no identifying details but in later contact they did put in my children’s names. They never addressed me by name.
Uncomfortable as we were happy being left alone.
It was dreadful! I am an extremely experienced home educator with over 15 years of experience, with my adult children demonstrating the beneficial fruits of our approach to education in their chosen careers and all of my children happy and thriving, all taking part in so many different events and activities, so most certainly not “”hidden””. I have managed very well without any contact from the council previously, and it has been so much easier not to have the nuisance of them trying to be involved. I am well aware of my rights as a home educator and so would have thought I would be able to handle any such coldcalling confidently, but I had not expected this to be such an upsetting, distressing and overwhelming experience. I feel angry, treated with suspicion, that my privacy and home are violated by such an intrusion. Pretty much the first thing one of the cold-callers said to me when I confirmed that, yes, I had children still of school age, was “”why did you not register them with us?””. As if this is already a requirement. She also asked for information that I know I am not entitled to provide, and gave me false information, conveying they have a duty to regularly monitor my provision when I know this is not their lawful duty. “
Two responses indicated that the initial contact was significantly less distressing and more acceptable when made by email rather than by cold-calling.
For example:
I received an email and was just asked to provide details of our home education journey so far. EHE officer was happy to keep all in writing and was satisfied with the details I gave. However I was/am very frustrated at the way in which my details were given to EHE officer.
Question 9, Figure 7: Whether council staff explained the source of identifying data.
86.4% of respondents were not told by the council where they had sourced their identifying data from.
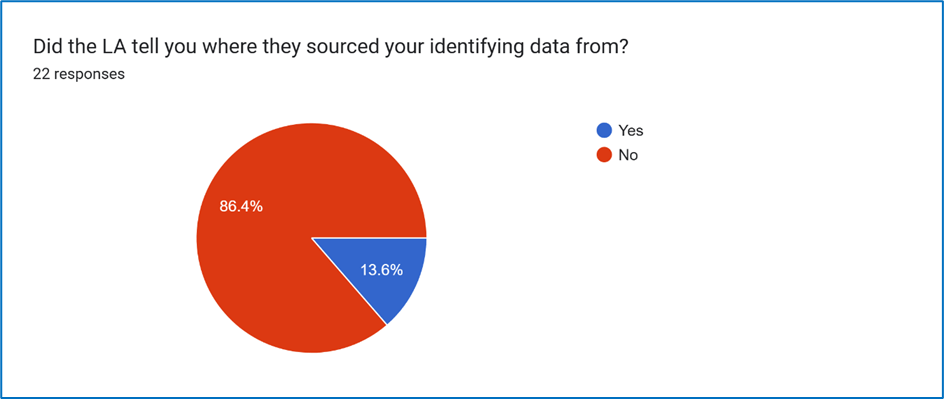
Figure 7:
Question 10: information given or not given by council staff on source of identifying data.
Some were not told the source, even on direct questioning. At least one respondent had to submit a freedom of information request to establish the source as being from the CME database pilot mechanisms. Two were told the source of their data was “confidential” or “anonymous”.
Concerningly, several respondents were given false or questionable information by council staff about the source of their data.
For example:
She said it was identified that my youngest (6) was not on a school register. But that does seem odd/irregular because my eldest aged 10 was also not on a school register and they didn’t flag that.
Told it was from the NHS which I do not believe as explained above
They said I contacted them informing them of my intention to HE, I did not.
In the very few instances where respondents were directly told that their data had been obtained as a result of the CME database pilot mechanisms, the inaccurate way this was conveyed potentially exacerbated the risks and negative consequences of these mechanisms.
For example, council staff stating that the information had come from “doctors”.
They said they had been doing a sweep on certain age groups, and had come round to the younger age, and told us they got the info from the Dr’s.
Question 11: Figure 8 enquiries about educational provision.
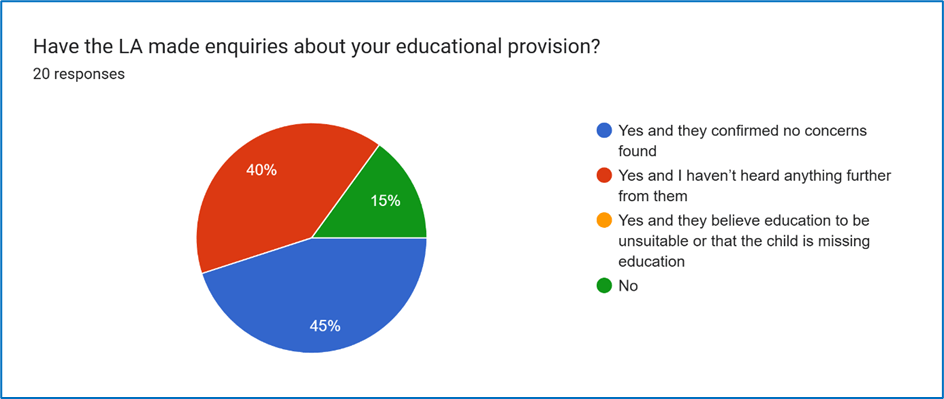
Notably, none of the families identified were found have children who were “missing education”. All of the families who were likely to have been identified via the so-called “CME” database mechanism were all home educating families not CME.
Question 12, Figure 9: were children placed onto CME databases and if so, were families aware.
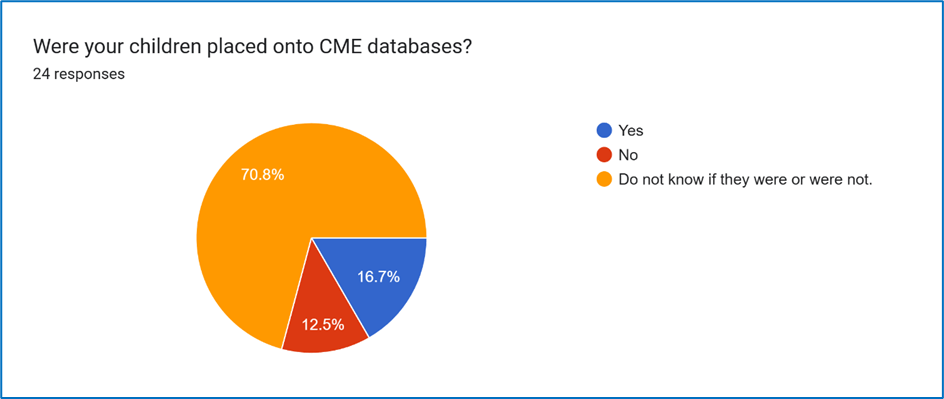
Even though no child was identified as missing education, as confirmed by Figure 8, it is notable from Figure 9 that that only 12.5% of respondents could feel reasonably confident in believing their child/children had not been placed onto these “CME” databases.
This relates to Welsh Government’s repeated attempt to give a different depiction to the meaning of CME and EHE from lawful definitions, in a manner to connote a role for the council that it does not lawfully have. This will be discussed later.
It should be noted that, according to the Schedule included in the consultation documents, a significant amount of personal information about the child, their education and their contacts would be expected to be stored on such databases.
Furthermore, only two respondents had been clearly told by the council that their children had been placed on these databases.
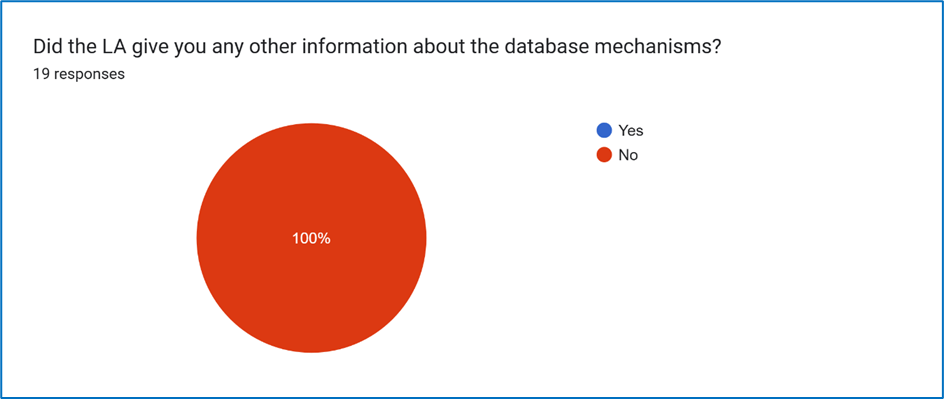
Question 13 Figure 9: lack of provision of information about the databases.
That concerning observation and criticism of the pilot is confirmed in Question 13 Figure 9, which demonstrates that no family were given any further information about the database mechanisms.
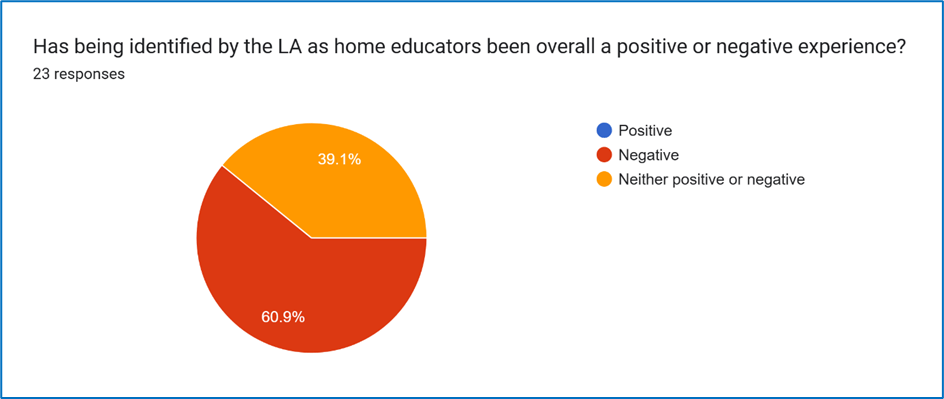
Question 14 Figure 10: lack of benefit for families of pilots and non-consensual datasharing.
The lack of benefit for children and families of non-consensual datasharing and the CME database pilot mechanisms was demonstrated in Question 14, Figure 10,
Where two thirds of respondents indicated being identified by the LA as home educators had been a negative experience, and no respondents found this to have been or become a positive experience.
Question 15: opportunity to comment further on the impacts of being identified by the LA as home educators.
These comments included:
I kind of feel always on edge, waiting for them to just jump out of the woodwork again when I least expect it.
As stated previously, I think an expectation that someone can turn up unannounced at your door with just a lanyard sets a dangerous precedent that could put children at risk.
If this is the culture & expectation created, then a child’s home is no longer a safe space because anyone could turn up pretending to be from a legitimate organisation & obtain confidential personal information.
Having to write a yearly report means more time is now spent on keeping education logs when I could spent that time on planning & preparing learning experiences instead
More admin writing reports and emails to people who I don’t think are qualified to judge home education
This whole process is insidious and alarming.
They not only obtained information without my consent, but they then used that information incorrectly to contact me about my very young child. They have also phoned multiple times after I asked for all communication to be made via email and insisted on home visits and samples of work from my older child.
Feels like overstepping as child is not even CSA yet.
This inconvenience and monitoring system does NOT create trust. I do not consent to my tax money being spent on a state nanny to monitor my children.
Negative because they’ve been very unclear
Honestly they haven’t given any information about where they found my details and they now say they will be in contact every year.
I feel like our home, our safe space was effectively violated by them sending a letter to our home. They turned up to a friend’s house and my children were worried they would do the same. I think it’s disgusting they are allowed to do this
I fear that there will be a style of monitoring that will encroach on the freedom of home education. I am concerned that families will be made to recreate school at home and create a standardised educational environment that was the exact environment our children were thriving whilst being away from.
I worried a lot about being ‘found’ but in reality it’s made no difference to anything so far.
I have attended one of the LA organised events with my children, however reading the research regarding the LA and how they like to “”keep eyes on the children””, I am unlikely to attend another one, out of principle!
Being observed inevitably negatively influences the freedom and discretion with which parents raise and educate their children. We have been free to let the children just learn and enjoy learning without pressures, demands or expectations, to follow their interests and passions, to be children. It is an approach that works so well, that allows children to thrive. My adult children are excellent examples of this, being considered “”successful”” by the kinds of measures that the school system looks for, but especially “”successful”” in being well-rounded, well-educated, articulate, informed people who play such wonderful roles in society and who still love learning and questioning.
Expectations of descriptions and analyses of what constitutes an “”educational experience”” and look for and document “”markers of progress”” inevitably negatively affects that process. It hinders and obstructs true learning. I am sorry that the council are going to try to impose monitoring onto us (even though I know they have no lawful duty to do so, but they try to do so through what they call “”annual reports). I am sorry not just because the time and hassle take me away from my children’s actual education, but because it will mean so, so much effort to try to prevent the pressures that that places on me as the parent from filtering down to be pressures on the children or to change their educational styles and provisions.
Question 16 Figure 11: opportunity to identify safeguarding risks, particularly based on the experiences of those that had been impacted.
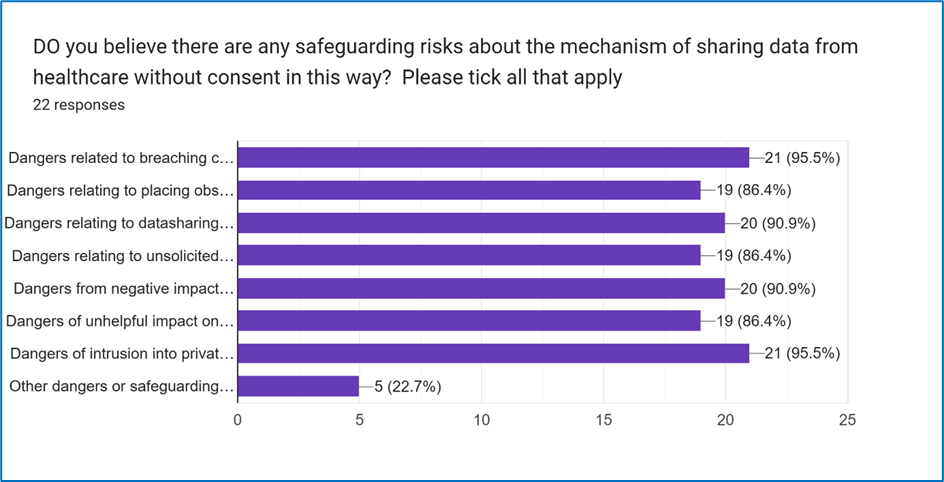
These results are also depicted in table form for clarity.
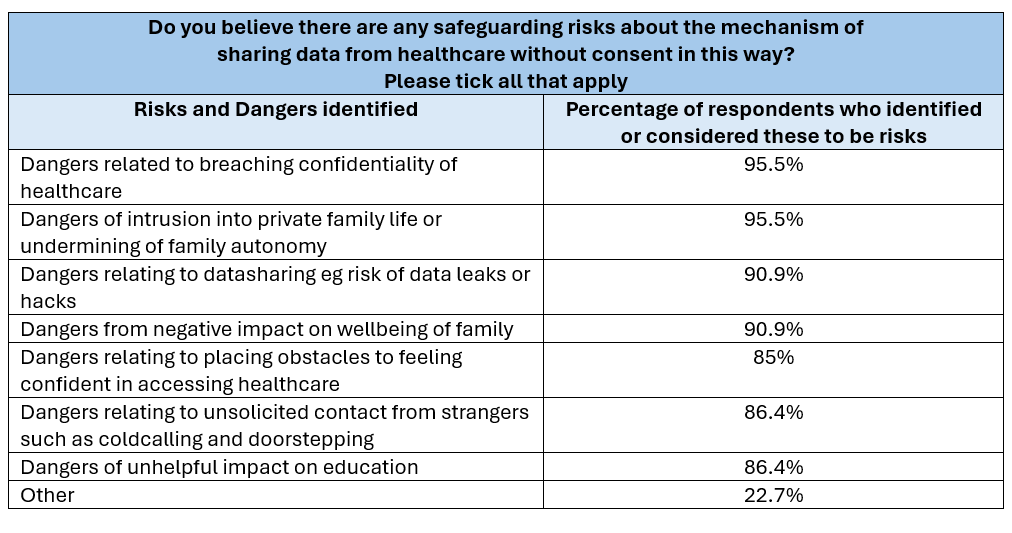
Opportunity was given to comment on other forms of safeguarding risks that respondents may feel or have found to be relevant to the CME database mechanisms.
These included:
- Dangers of false reports being made against a family.
- Concerns at what the data would be used for
Who knows what this government will do with are child’s information. It begs the question ‘who else are they sharing our data with, and what data’.
We don’t know where they received the information. There wasn’t enough detail in the initial letter to even confirm it was legit
- There were further comments on the impact on confidence in accessing healthcare. For example:
Education and healthcare should be entirely separate…It almost makes me concerned, if my child was ill and had to go to hospital, for example, would I then have the LA showing up telling me that my child has to go to school now?? It sounds irrational, but that’s the kind of fear data sharing invokes.
Damages patient- provider confidentiality as in my opinion where there are no safeguarding concerns data should not be shared, families should be allowed privacy and those outside of healthcare should not be accessing patient data.
The mechanism was considered to
“create a safeguarding risk”
with one respondent commenting that it was
“not a well though through decision”
ironically but also with relevance adding that
“The people who made this scheme clearly weren’t home-ed”.
Question 17 Figure 12: Complaints
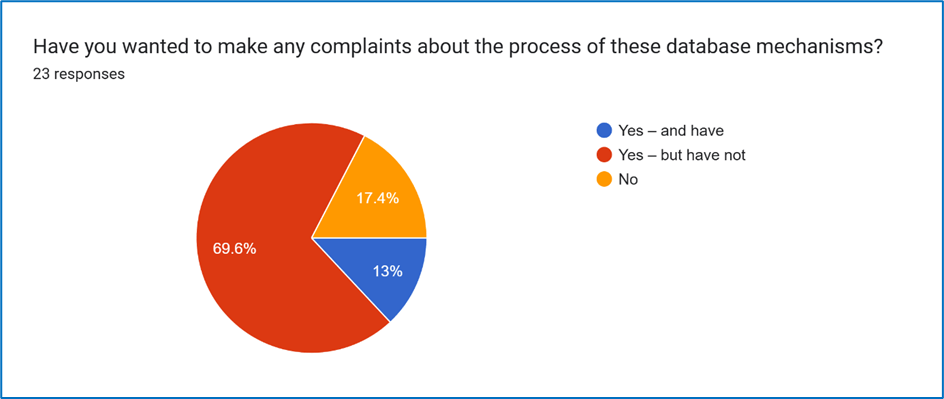
Only 17.5% of respondents had not considered making a complaint about the process of database mechanisms.
Further comments on whether or not people had decided to complaints in relation to CME databases and/or related issues with their data being shared with the council included: Concerns about “tracking” of families and “discrimination” in the subsequent use of the data, with several respondents referring to “lack of trust” in the council in relation to these database mechanisms.
Local councils have repeatedly suffered from data breaches, I believe it’s unacceptable for them to hold such confidential & sensitive information on our children. They simply cannot be trusted to keep such data safe.
Any child actually missing education will be pushed further under the radar.
It is overstepping in a damaging way for families that have only ever done the best for their child. If you share data, there should be very valid reasons for doing so. We should always be informed about the sharing of data.
It’s underhanded and unethical. I would have appreciated an email or phone call before people showing up at my door unannounced, making threats.
I think it’s a breach of privacy. I also think it’s the easiest and cheapest way that they have to look like they are doing something while actually doing nothing of consequence.
I think it’s disgusting. It’s a huge invasion into our homes, our privacy and our children’s lives.
Absolute disgrace
I believe it is abhorrent, unethical, immoral, and so obviously counterproductive.
Saying want to find “vulnerable children” and yet placing deterrents to those children accessing healthcare?
It is such a ridiculous lack of insight and understanding, that you just couldn’t make it up.
In most other situations, full consent would be needed to share information such as this. Once again, we are being discriminated against based on a choice we have made in regards to our children’s education.
Further discussion and observations
The CME database mechanisms being used to identify responsible home educators who had quite lawfully not informed the council of their families’ mode of education, rather than being an efficient, safe or appropriate tool to identify children who are CME, is exactly what home educators anticipated the effect, and indeed the reason, of these databases to be.
This is exactly what home educators anticipated the effect, and indeed the reason of these databases to be, namely to be an attempt to monitor and oversee law-abiding responsible families.
Ms Neagle’s department repeatedly claimed, especially during the consultation process for CME databases, that these databases mechanisms did not relate to home education. However, it is clear from the design of the mechanisms as well as from previous statements including former Cabinet Secretaries for Education that these were designed to identify home educating families.
The Welsh Government have repeatedly attempted to use these CME databases to convey incorrect definitions of “CME” and home educated, implying that children are only home educated if the council know that they are and approve of this. That is not the legal status, home education is the default setting, with parents needing to opt out of this to proactively register a child in a school should they choose to do so. Should families choose to deregister a chid from school to be home educated, the documentation codes used are for home education, not for CME.
A further example of the misleading definitions of CME and EHE that the Welsh Government have sought to convey was noted in the recent comments of the present Cabinet Secretary for Education to the Children, Young People and Education Committee.
In that meeting, Ms Neagle also referred to the pilots of those “CME databases” as “particularly challenging”, interestingly commenting that this was “what we thought it might” be.
Concerningly however, she stated she was “looking forward” to the evaluation that she says is under way at present, stating that, despite the challenges, she intends “to see how we could take that work forward”.
Note the use of the term “how,” not “if”.
When considering the modes of initial contact chosen by council staff it is helpful to compare and consider not only the feelings expressed by the respondents to this survey, but also those expressed by another recently conducted survey of the experiences of Welsh Home Educators in relation to LA conduct, alongside the views expressed by council staff in the Welsh Government commissioned evaluation of their EHE guidance.
That survey demonstrated the detrimental and counterproductive impacts of cold-calling and doorstepping by council staff, which contrasts to the perceptions of council staff of how families consider such cold-calling, as stated in the WG-commissioned evaluation of their guidance.
The observations of lack of transparency, accuracy and accountability, as demonstrated in this survey, alongside a recent survey of the general experiences of home educators in relation to LA conduct and WG policy, run counter to the principles of GDPR and good practice in data management.
It is difficult for families to challenge any inaccuracies in databases such as these CME databases, if they are not even informed their children are or were on these, let alone permitted to see what is stored on such databases.
It is also notable that, as for any other areas of council policy or practice in relation to home education, there are no independent complaints, appeals, mediation, advocacy or tribunal services or mechanisms to address problems with policy or staff conduct in relation to home educated families.
The Data Protection Impact Assessment (DPIA) for the CME database mechanisms was only published after the consultation was closed. The DPIA contains numerous misleading comments and points that require constructive criticism, too many to list here. A critique and rebuttal of this DPIA is presently being drafted.
This survey also highlights a range of risks to the safety and wellbeing of children in Wales of the use of such mechanisms, risks that were not addressed in the WG-commissioned evaluation of these.
These risks and consequences were however raised in the many responses to the consultations on these measures, including by professional bodies as well as those with lived experience,
but the Welsh Government chose to overlook these warnings.
This is somewhat ironic, given the present Cabinet Secretary’s previous comments in the Senedd that
“You cannot have a consultation and then just ignore that consultation.”
The unreliability of data used by council staff in these CME database pilots, as noted in areas of this survey, is mirrored in the WG-commissioned evaluation of these pilots.
A key concern of those who had attempted to warn the Welsh Government of the risks, damage and consequences of these pilot databases was, given how clearly unworkable these pilots appeared to be, which has now been verified by the WG commissioned evaluation of them,
that the underlying motivation for persisting in enacting legislation to undertake these was not so much to identity children who are allegedly CME,
but rather as an opportunity to introduce and then normalise datasharing from confidential NHS sources for non-healthcare purposes.
This clearly raises considerable ethical implications as well as potential safeguarding concerns.
It would obviously be inappropriate to take any further action in relation to any aspects of these CME database pilots until there has been full evaluation of the impacts, risks, consequences and experiences of those affected, as well as input into the ethical implications and repercussions on clinician-patient relationships of non-consensual data-sharing from healthcare sources.
We trust that, moving forward, future Welsh Governments and Senedd Members would engage fully with members of the community and be willing to appreciate their experiences and insights before developing policies and practices that relate to them
